Mary Ann R. Garcia, DNP, MSN, RN, Chamberlain University
Diabetes is a major public health problem worldwide. It is characterized by an increase in blood sugar levels and may manifest as either Type-1 or Type-2 diabetes mellitus (American Diabetes Association [ADA], 2018). Diabetes poses a significant economic burden due to its high diagnostic and treatment costs. In the year 2017, $327 billion were utilized in the diagnosis of diabetes (ADA, 2018). Additionally, more than 2.4 million residents of the state of Florida are diabetics, with more than 5.8 million people being confirmed to be in the early stages of diabetes development (Tabák, Herder, Rathmann, Brunner, & Kivimäki, 2012). These figures are more than double that of diabetes prevalence of the past two decades (Dabelea et al., 2014).
Current approaches in the management of diabetes involve continuous participation in a multifaceted program aimed at reducing and preventing further complications associated with the disease (Boels, Vos, Metzendorf, & Rutten, 2017). This is because diabetes is a complex and chronic illness requiring consistent patient-oriented management education, which is essential in precluding acute complications and reducing the risk of long-term complications (ADA, 2018). Diabetes self-management education (DSME) and diabetes self-management support (DSMS) are programs central to the management of diabetes (Boels et al., 2017). Collectively, these approaches are known as the Diabetes Self-Management Education and Support program (DSME/S), which forms the essential basis for self-management in individuals with Type 2 diabetes mellitus. This project will focus on the use of mobile devices as a strategy towards implementing the Center for Disease Control and Prevention (CDC) guidelines on managing diabetes and facilitating the DSME/S program at the Patient's Choice Primary Care Associates Clinic in Florida County, Florida.
Problem Statement
One of the ongoing challenges that have been faced by healthcare practitioners is to provide care and support that aims at producing and sustaining the desired improvements in the health of people diagnosed with chronic diseases such as diabetes. The development and implementation of the Diabetes Self-Management Education and Support program (DSME/S), as recommended by the CDC, provides diabetic patients with the necessary knowledge and skills for the effective management of diabetes and prevention of diabetic-related complications. However, the patient’s non-adherence to diabetes management plans coupled with inadequate health professional manpower has resulted in an increase in the incidence of diabetic-related complications.
Diabetes is a chronic condition that requires the patients to receive continuous medical care and self-management education to aid in preventing severe complications and also in reducing the risk of long-term complications. Research that has been conducted on technology-based self-management, such as the use of messaging services to educate patients on diabetes self-management, has provided evidence that the use of technology in managing diabetes is effective (Holmen, Wahl, & Småstuen, 2017). This project will seek to answer the question, “Does an 10-week interventional use of mobile devices, compared to the current practices of implementing the CDC’s guidelines for self-care management, improve patient scores on the diabetes self-management questionnaire?”
Significance of the Problem
Diabetes has become a shared chronic condition that affects millions of people in the United States. The patients' non-adherence to diabetes management plans was the problem identified by the project manager and the primary care center’s administrator which resulted to an increased incidence of diabetes-related complications. Diabetic patients need thorough, continuous assessment and care by healthcare providers. Despite the adoption of national and local guidelines for the management of diabetes, the implementation strategies have not yielded desirable outcomes. Globally, the effective management of diabetes requires a patient to make a number of daily self-assessments for the efficacious management of his/her health. The DSME is an important channel through which people with diabetes acquire the necessary knowledge and skills to better manage their health. It is through DSME programs that diabetic patients are continuously assessed and taught the appropriate health management skills needed to accurately self-manage by addressing the patient's health literacy as well as needs, physical limitations, and emotional concerns. Therefore, it is important to evaluate the extent and effectiveness of the implementation of DMSE programs.
Diabetes self-management education (DSME) has been proven to be cost-effective in decreasing the number of hospital admissions and readmissions due to diabetic-related complications. As a result, DSME has great potential to significantly reduce the diagnostic costs associated with the treatment of diabetic-associated disorders (Powers et al., 2015). This is achieved through blood glucose control, low blood pressure, and normal cholesterol levels. Other interventions include impacting the patient's behavior, such as drafting a regular workout plan and healthy food choices so as to reduce body weight, and impact behavior by rehabilitating vices, such as smoking, and encouraging strict monitoring of blood glucose levels and the appropriate use of insulin. It is through these interventions that diabetic patients have been able to experience lower occurrences of complications and improved psychosocial well-being.
The advances in modern-day technology provide immeasurable avenues for tackling problems that have risen due to globalization. These technologies can be harnessed and used to deliver DSME right at the point of care and thus improve diabetes self-management. One such advancement is with mobile technology, which is a low-cost and easily accessible means for both healthcare providers and patients to share DSME information regardless of time and space. Consequently, this technology is far-reaching and is able to impact people in areas where programs are not readily available.
The Center for Disease Control and Prevention (CDC) advocates for participation in self-management education (SME) programs that aid diabetic patients in learning skills in diabetes management (CDC, 2018). The DSME is provided by a healthcare professional as a tool with emphasis on disseminating the knowledge and skills imperative for diabetes self-care. Self-care education has been proven to be effective in the management of chronic conditions. These programs have been incorporated into DSME where patients are equipped with the knowledge and participated in activities aimed at controlling blood sugar levels and preventing complications.
Synthesis of the Literature
Burke, Sherr, and Lipman (2014) stated that an estimated one out of three Americans is either affected by or at risk of being affected by diabetes mellitus. Globally, the number of individuals with diabetes has grown exponentially and is estimated to rise further, with estimates predicting that the number will surpass 550 million by the year 2030. Diabetes self-management education (DSME) is considered the cornerstone in the clinical management of diabetes and aims to increase patients’ knowledge, skills, and self-management behaviors regarding their disease (Harris, Silva, Intini, Smith, & Vorderstrasse, 2014).
Mobile phone short message service (SMS) messages are being used increasingly to deliver interventions designed to enhance healthy behavior because the majority of people worldwide own a mobile phone, regardless of socioeconomic status; all mobile phones support SMS messaging; and SMS messages utilize push technology that enables outside parties to initiate contact with mobile phone users (International Telecommunication Union [ITC], 2013). Mobile phones have been used effectively to support healthy behavior adoption and disease management. The prospective, randomized, primary prevention trial study of Ramachandran et al. (2013) on Indian workers with impaired glucose tolerance utilizing a mobile phone messaging intervention proved that mobile phone messaging is a useful and acceptable method to deliver lifestyle modification to prevent Type 2 diabetes high-risk individuals.
Dobson et al. (2015) conducted a non-randomized pilot study that aligns with previous text message–based interventions in people with diabetes. In this mixed method, a tailored text message–based diabetes support intervention called Self-Management Support for Blood Glucose (SMS4BG) was developed. The study established that SMS4BG is an acceptable and potentially useful tool for adults with poorly controlled diabetes.
The systematic review conducted by the team of Garabedian, Ross-Degnan, and Wharam (2015) suggests that healthcare providers are more likely to use mobile health (mHealth) if reimbursed by payers. The utilization of mHealth apps aid in promoting behavioral change and improving the health outcome of patients with diabetes. Medicare, the largest public payer in the United States and the standard-setter for many private payers, provides insufficient reimbursement of telehealth services and has no mechanisms to pay providers for interacting with the vast majority of the mHealth technologies in this review. In addition to broader reimbursement for telehealth, the movement toward outcomes-based payment models might encourage investment in mHealth in an attempt to promote efficient, high-quality care and management for chronically ill patients.
The meta-analysis review by Orr and King (2015) indicates that SMS messages alone have a small, positive effect on healthy behavior and that multiple SMS messages per day may enhance the effectiveness of SMS message interventions. As the age of health consumers did not impact the effect of SMS message interventions, this suggests that SMS message interventions are effective across age groups. SMS messaging is a simple, cost-effective intervention that can be automated and has the potential to reach anyone, with any mobile phone, anywhere in the world.
Mobile phone technology has been shown to have full acceptance across various age groups and socioeconomic groups. This is supported by the randomized controlled trial research done by the group of Pludwinski, Ahmad, Wayne, and Ritvo (2016). They investigated the experience of individuals from a lower income neighborhood who were diagnosed with Type 2 diabetes mellitus (T2DM) to compare the effectiveness of six months of smartphone use with health coaching vs. health coaching of equal intensity without smartphone support. The findings of the study suggest that interventions with T2DM assisted by smartphone software and health coaches actively engage individuals in improved hemoglobin A1c (HbA1c) control. However, the study also identified frustrations in managing chronic conditions with a particular focus on (a) medication and blood glucose; (b) diet/weight; and (c) comorbidities (Pludwinski et al., 2016). According to the article, people with diabetes can benefit from healthcare practitioners in their self-management (Holmen et al., 2017). The smartphones and applications offer a unique platform that can be utilized for communication where the applications can be integrated with healthcare information. Self-management interventions are crucial since they help to understand change.
The integrative review by Hunt (2015) indicates that technology can be utilized to complement healthcare provider diabetes care by providing both motivational and educational support. According to the study, technology offers a platform where patients diagnosed with diabetes can be educated on new routines and practices related to diabetes management. The use of technology can support daily diabetes self-management activities that include problem solving, monitoring for complications, taking medication, healthy eating, exercising, and blood glucose monitoring.
The systematic review done by Shah and Garg (2015) highlights the numerous methods that have been developed for self-management of diabetes due to technology development. The researchers indicated that there is a significant increase in the prevalence of diabetes worldwide. Poor control of blood glucose can lead to an increase in healthcare expenditures and higher rates of diabetes-related complications. The researchers reported that the recommended glycosylated hemoglobin (HbA1c) should be 7 or less to avoid diabetes complication and self-management education is significant in helping to attain this goal. According to the authors, the number of smartphones and broadband in the market were expected to increase by 2018, which can make it possible to use mobile app technology to educate patients on how to better manage their diabetes. The researchers indicated that due to the rising number of people being diagnosed with diabetes and due to an inadequate number of healthcare professionals and lack of adequate resources in developing countries, there a need for the development of a cost-effective tool for diabetes self-management education to enhance diabetes outcomes.
Diabetes Self-Management: Impact on Healthcare
As a widely available, low-cost technology, mobile phones are a promising tool for use in engaging patients in behavior change and facilitating self-care between visits. The quantitative study by Nundy et al. (2014) offers early evidence that mHealth can enable healthcare organizations to adequately support patients beyond the traditional healthcare setting and achieve the triple aim of better health, better healthcare, and lower costs. The total cost of healthcare declined by $812 per participant per six months. This research reflected a net cost savings of 8.8% in costs for outpatient, emergency department, and inpatient visits. This study also suggests that mhealth diabetes programs hold promise for supporting chronic disease self-care, improving clinical outcomes, and reducing costs.
A retrospective analysis was performed by Brunisholz et al. (2014) for adult type 2 diabetes patients who received DSME training in 2011–2012 from an accredited American Diabetes Association center at Intermountain Healthcare (IH). These patients also had a glycosylated hemoglobin (HbA1C) measurement within the prior 3 months and 2–6 months after completing their first DSME visit. The study resulted in a threefold decline in HbA1C of the DSME patients compared to the control group. This study also demonstrates that patients receiving DSME within an American Diabetes Association (ADA) center are 1.5 times more likely to improve their five-part diabetes bundle score within 6 months. Improvement in the bundle score has the greater clinical benefit to the patients, may be less costly, even for those with multiple comorbidities, and is more efficient in practice than just improving one key marker—HbA1C—for diabetes.
A quasi-experimental study conducted in Chicago revealed that the use of mhealth services in following up diabetic patients showed an improvement in their blood sugar levels, a reduction in diagnostic cost, and an increase in patient satisfaction (Dick et al., 2014). Therefore, mobile phones are a promising platform for engaging patients in chronic care because most patients own and regularly use them. This study is also supported by a randomized control trial which revealed that patients are able to conveniently and instantly receive information targeted at improving their health outcomes via text messaging, calls, and mobile applications. Likewise, patients are able to share information with their healthcare provider in real time (Wojcicki, Ladyzynski, & Foltynski, 2013).
Project Design and Methods
The project was to enhance the primary care center’s existing practice through the integration of mobile services in educating patients and motivating them to be accountable for their own health. The project aimed to evaluate the efficacy of executing the CDC guidelines on diabetes self-management education through technology like mobile phones. The project aids in increasing the patient's level of self-management to prevent diabetic complication dominance and potential hospitalization.
Data Collection Procedures
As discussed in the previous section, the evaluation of the project was based on a pre-interventional and post-interventional DSMQ. It is noteworthy that this evaluation tool produced nominal data because variable labels are considered significant. In the DSMQ the items on self-care activities are answered through four options: “Applies to me very much” = 3, “Applies to me to a considerable degree” = 2, “Applies to me to some degree” = 1, and “Does not apply to me” = 0. The survey questions related to self-care activities; only the degrees of relevance were considered significant for evaluating the impact of the intervention. As such, the answers did not require any specific order for the level of relevance. Nonetheless, during the collection of the nominal data, the analysis of the data was based on the related labels (i.e., 0, 1, 2, 3). For instance, when the participants responded to the DSMQ and selected “Applies to me to some degree,” the recorded data was “1.” This helped quantify and answer the PICOT question.
The project question was answered using the simple t-test. The t-test is a parametric evaluation that provides information related to statistical inference concerning the population (diabetic patients) by establishing the statistical significance of the sample (Kim, 2015). This analysis assumes that the variables are obtained from a normal population. In the project, the current intervention and the use of mobile devices in the implementation of the DSME need to be compared, thus were making this analysis crucial.
Instrumentation
The DSMQ was used in the project evaluation. The DSMQ is a psychometric instrument, which was used to examine the patients’ diabetes self-management (DSM) activities (Schmitt et al., 2016). Notably, the scale used in this tool is effective in assessing self-management activities. The comprehensive and brief structure of the DSMQ makes it a suitable instrument in assessing the DSM dynamics on the subjects before and after the intervention (Schmitt et al., 2016).
The DSMQ tool entailed 16 items that covered five unique elements of diabetes self-management (DSM). All the DSMQ’s items were developed as behavioral descriptions from a patient’s perception. When the DSMQ was administered, the participants were expected to rate the degree to which each item was relevant to their case on a four-point scale (“Applies to me very much” = 3, “Applies to me to a considerable degree” = 2, “Applies to me to some degree” = 1, and “Does not apply to me” = 0). A transformation of the items scores was done to ensure that high scores depicted a desirable DSM behavior (and hence required reverse-scoring of items that were keyed negatively) and transformed or summed to five-scale scores within a range of 0–10 (Schmitt et al., 2016). The resultant scale reflected the participant’s medication adherence using two items, dietary control using four items, blood glucose monitoring using three items, physical activity using three items, and healthcare provider contact using three items. Lastly, one item exists, on diabetes self-care, which collects information related to the patient’s overall rating of diabetes self-care. The instrument utilized can be found in Appendix A.
Results and Discussion
This section describes and summarizes the quantitative analysis used to evaluate the research questions presented previously. Specifically, this section includes the results of the pre- and post- analysis of the DSMQs including both descriptive statistics and results of the repeated measures t-test.
Subscales of the DSMQ
The DSMQ is a standardized instrument that consists of 16 individual items related to diabetes self-care and management (Schmitt et al., 2013). Instructions for the instrument were as follows: “The following statements describe self-care activities related to your diabetes. Thinking about your self-care over the last 10 weeks, please specify the extent to which each statement applies to you.” (Schmitt et al., 2013). Respondents answered each question on a 4-point scale. Scale responses range as follows: “Applies to me very much,” “Applies to me to a considerable degree,” “Applies to me to some degree,” and “Does not apply to me.” Of the 16 items on the DSMQ, 7 were scored positively and 9 inversely (reverse scored). The 9 reverse-scored items were re-coded in SPSS as per the DSMQ scoring manual.
Following data scoring, the relevant subscales of the DSMQ were created. Briefly, the DSMQ consisted of four subscales and an overall “sum score.” The subscales were labeled as follows: “Glucose Management” (items 1, 4, 6, 10, 12), “Dietary Control” (items 2, 5, 9, 13), “Physical Activity” (items 8, 11, 15), and “Health-Care Use” (items 3, 7, 14). Item 16 is the “Sum Score” that provides an estimate for the overall self-care rating of an individual participant.
Major Findings
The Statistical Package for the Social Sciences (SPSS) version 25 computer software was used to analyze the data from this study. The paper-and-pencil survey results were entered directly into the SPSS software and checked for accuracy to ensure that (a) all data were entered correctly and (b) each participant’s pre- and post-test were matched correctly.
The primary research question explored in this study was, “For adult patients with Type 2 diabetes at Patient's Choice Primary Care Associates Clinic, does the implementation of the CDC guidelines for self-care management through the use of mobile devices improve scores on the diabetes self-management questionnaire, compared to current practice in 8–10 weeks?” Given that the study collected pre- and post-intervention data for a single group of participants, a repeated measures t-test was the appropriate data analysis technique. Repeated measures t-tests were run on the four subscales and the overall summary score for the DSMQ. Table 2 presents the repeated measures t-tests were run on the four subscales and the overall summary score for the DSMQ.
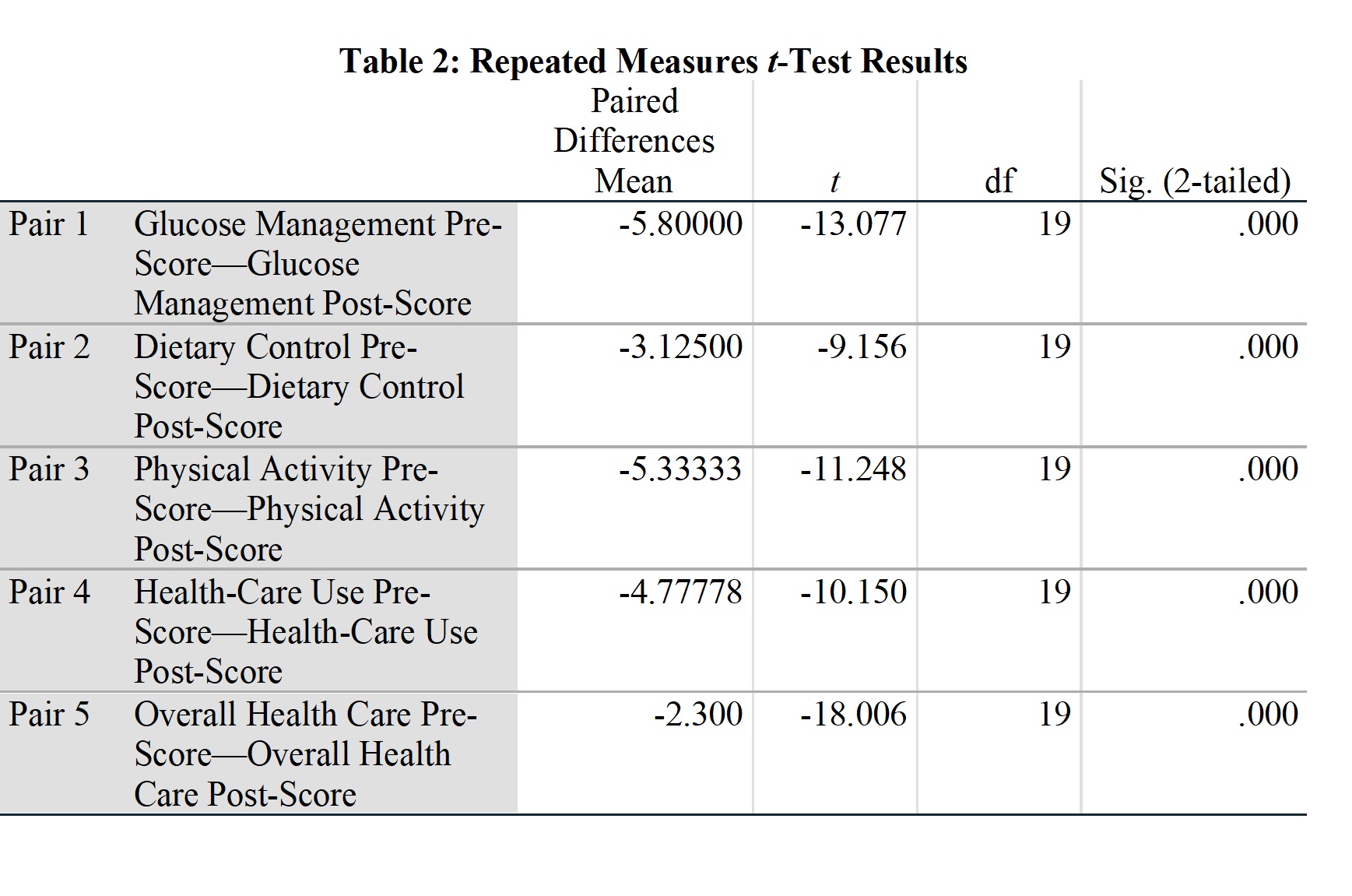
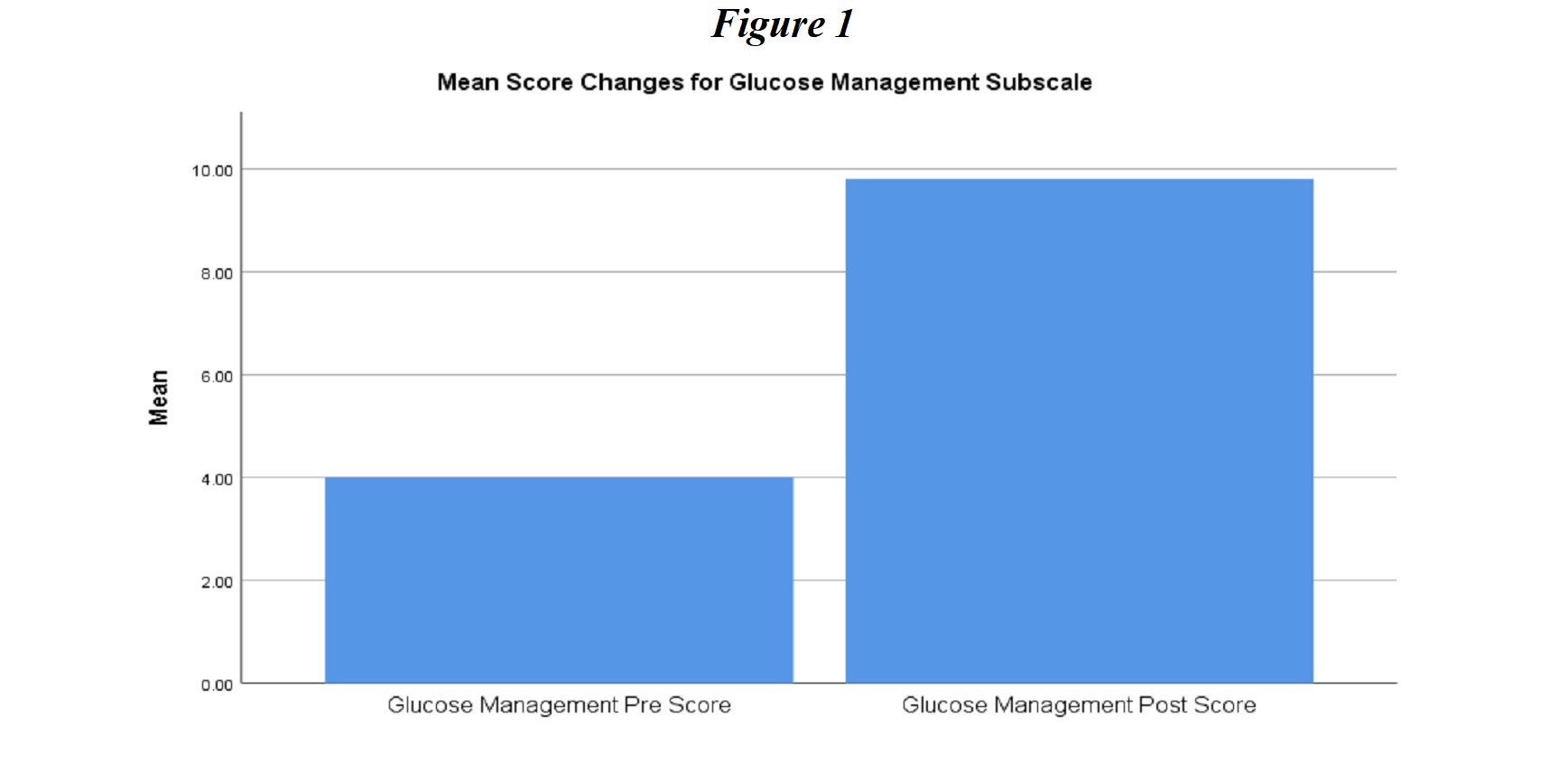
Glucose management. The first subscale of the DSMQ analyzed in this study looked at responses to questions related to the regularity of self-monitoring of blood glucose. Figure 1 shows repeated measures t-test results indicated that patients rated their glucose management practices significantly higher post-intervention, indicating that they were more likely to practice positive behaviors to maintain their blood glucose level (pre-test Glucose Management score N = 20, M = 4.00, SD = 1.87; post-test N = 20, M = 9.8, SD = 0.488), t(19) = -13.08, p < .05).
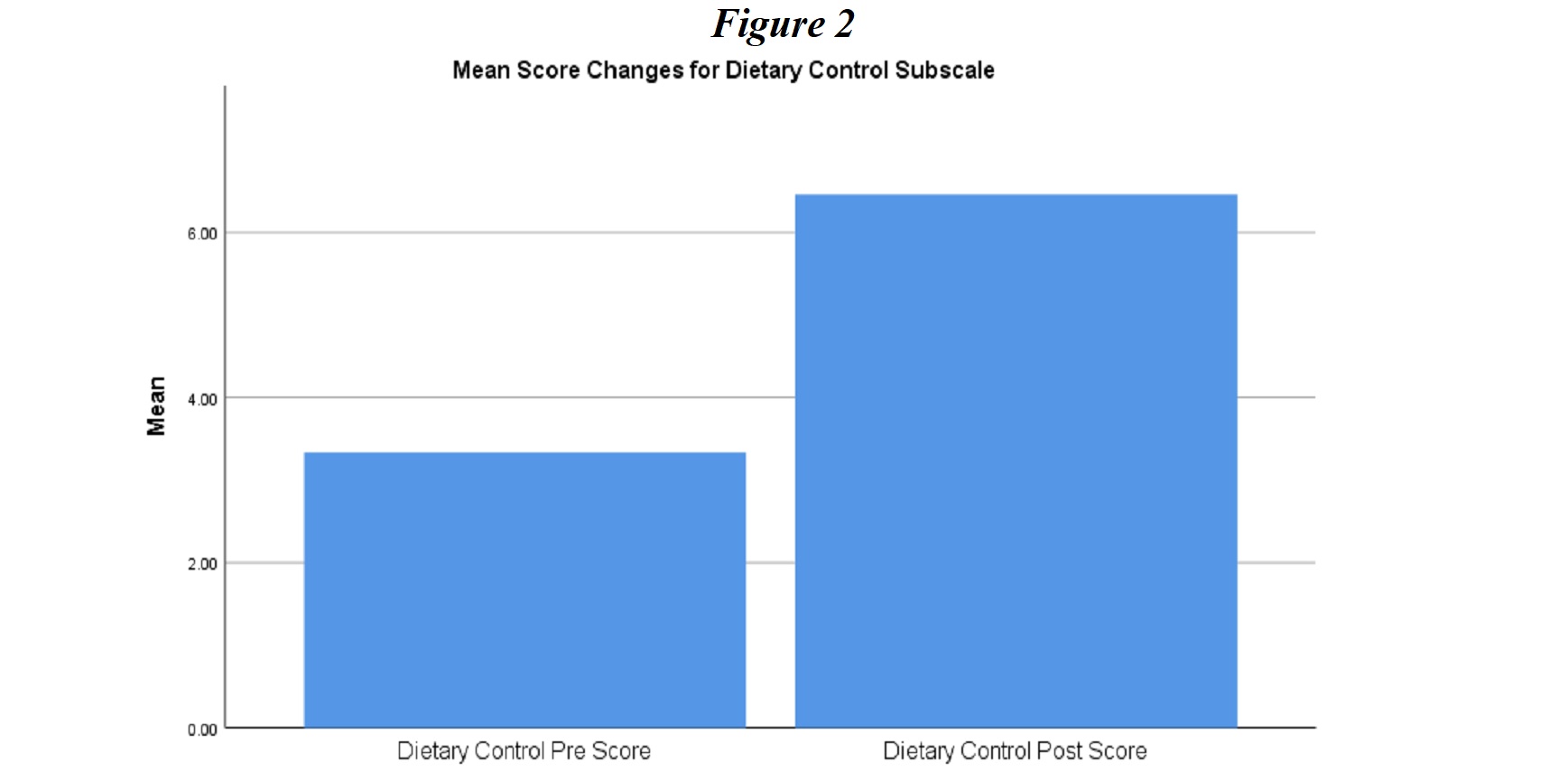
Dietary Control. The second subscale of the DSMQ analyzed in this study assessed diabetes-related aspects of diet (e.g., eating foods that affect glycemic indices, following doctors’ recommendations for diet and alcohol consumption). Figure 2 indicates that participants had significantly better dietary habits post-intervention (pre-test Dietary Control score, N = 20, M = 3.33, SD = 1.48; post-test N = 20, M = 6.46, SD = 0.756, t(19) = -9.16, p < .05). The participants had many challenges and questions in understanding food preferences and preparation when they were sent the Eating Well series text messages. Different strategies were applied during the implementation phase, which included follow-up calls, series of text message on quick tips on reading food labels and grocery shopping, and also provided visual handouts that were available from the clinic. This approach was supported by the study of Orr and King (2015), which indicates that short messaging service (SMS) alone has a small, positive effect on healthy behavior and that multiple SMS messages per day may enhance the effectiveness of SMS message interventions.
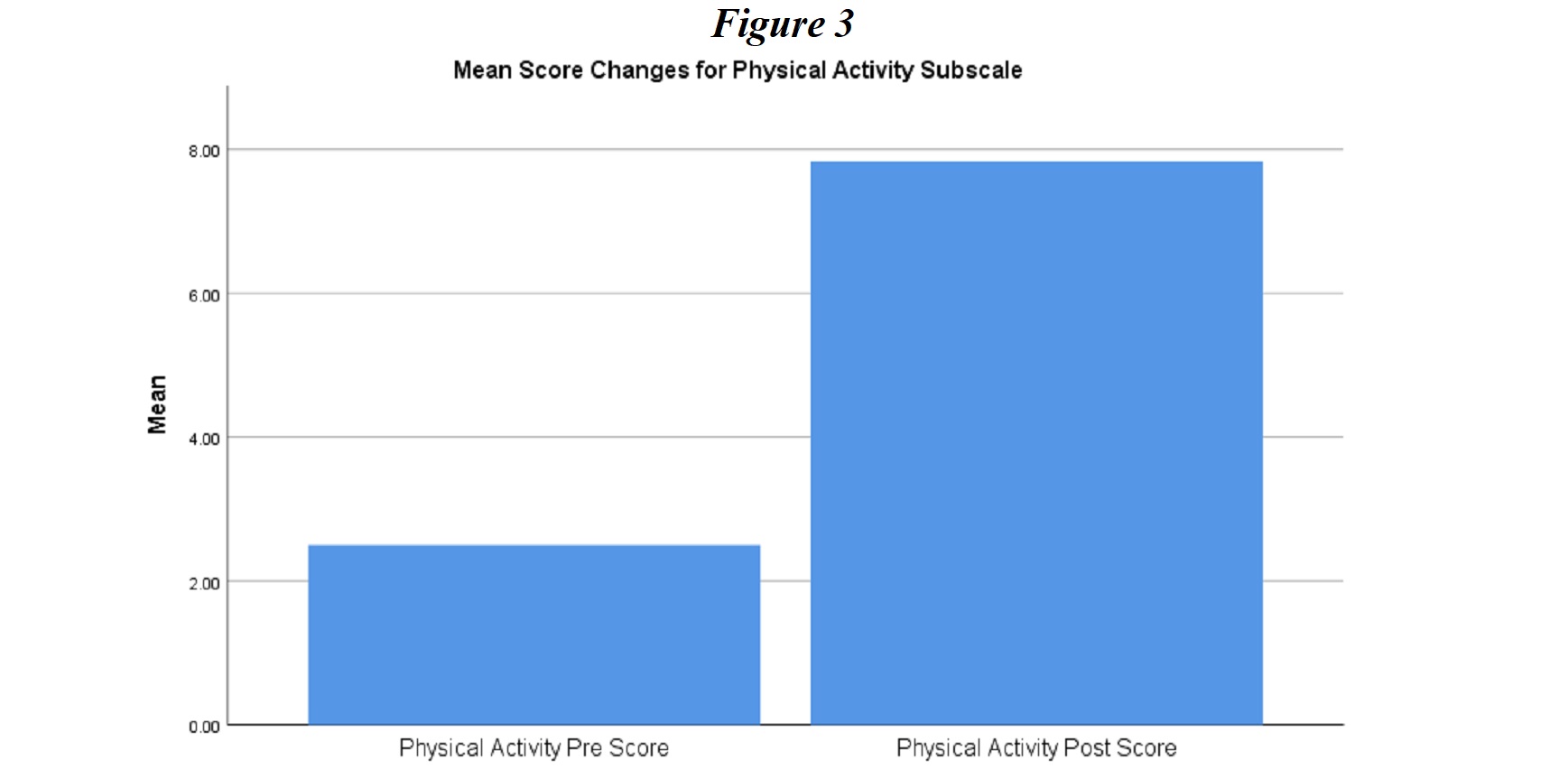
Physical Activity. The third subscale analyzed presented responses to questions related to the regularity of physical activity. In Figure 3, repeated t-tests yielded results indicating that participants were significantly more engaged in physical activity post-intervention as presented in Figure 3 (pre-test Physical Activity score, N = 20, M = 2.50, SD = 1.48; post-test N = 20, M = 7.83, SD = 1.46), t(19) = -11.25, p < .05).
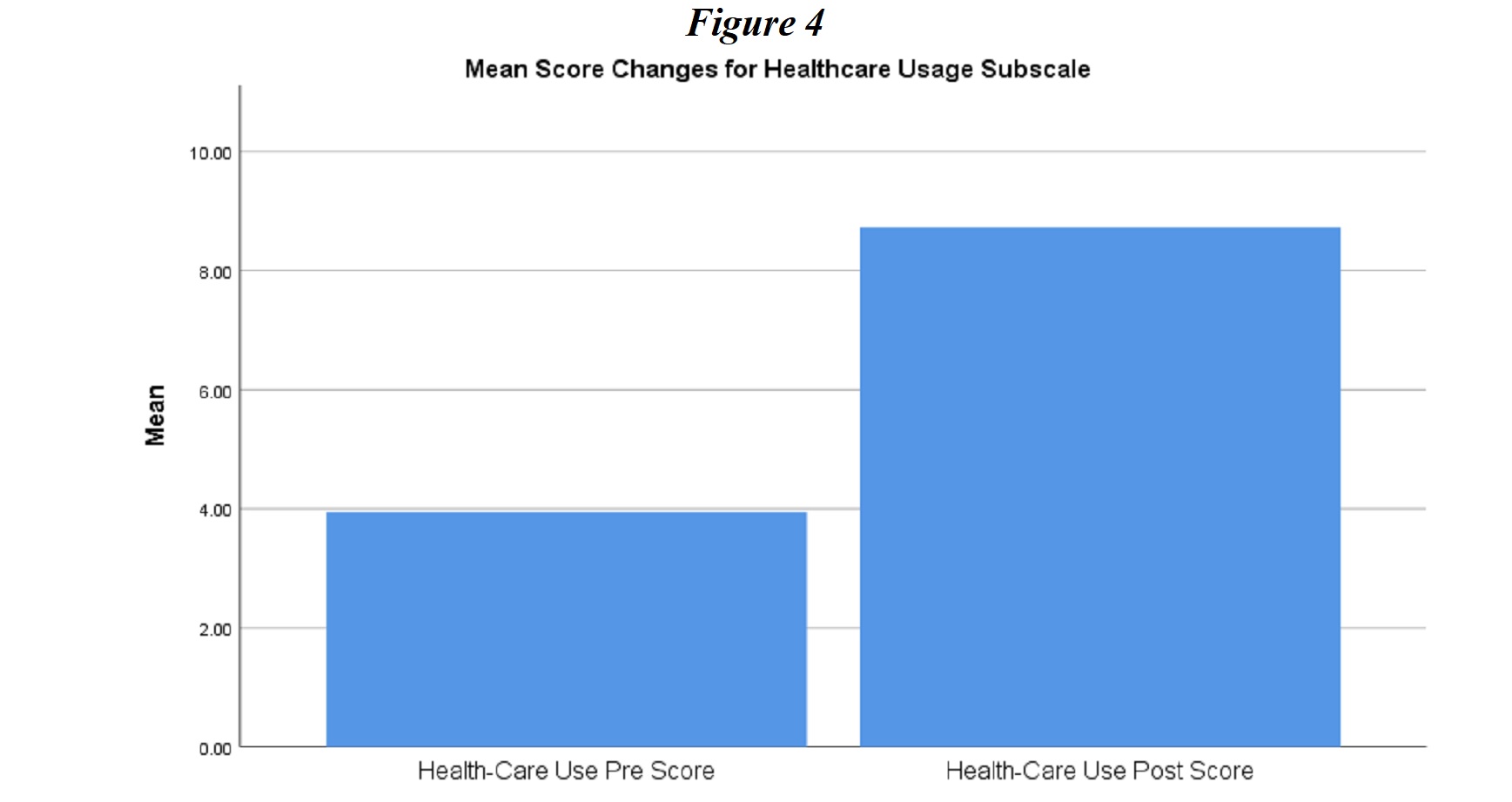
Healthcare Usage. The last subscale analyzed in this study examined participants’ adherence to appointments with healthcare providers for their diabetes management as shown in Figure 4. Repeated measures t-test results indicated that participants were significantly more engaged in the healthcare appointments and more likely to attend follow-up visits with healthcare providers after the intervention (pre-test Healthcare Usage score, N = 20, M = 3.94, SD = 1.67; post-test N = 20, M = 8.72, SD = 1.26), t(19) = -10.15, p < .05).
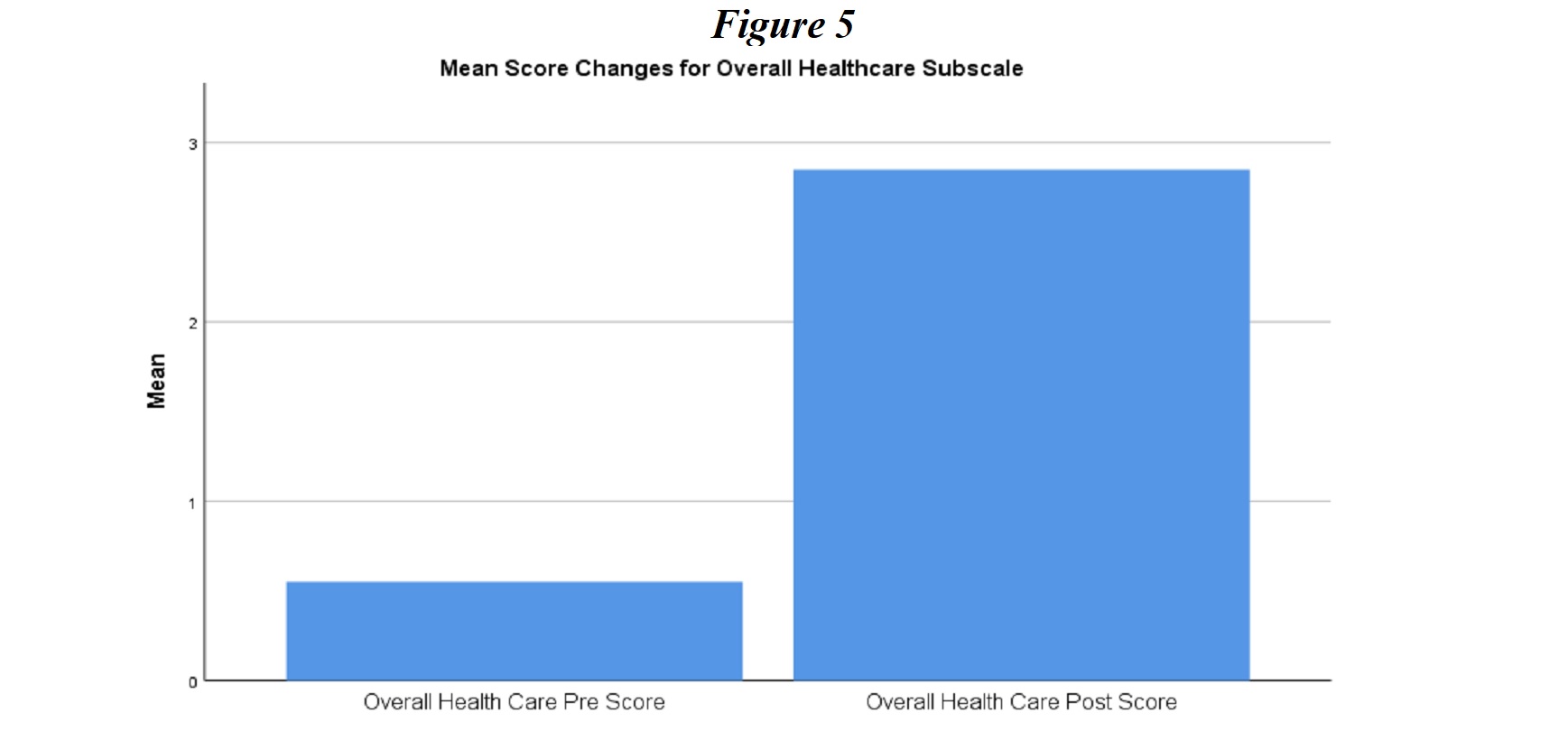
Overall Self-Care. The final item analyzed in this study looked at overall self-assessment of the participants’ diabetes management presented in Figure 5. Repeated measures t-test results indicated that participants’ self-assessment scores were significantly higher following the intervention (pre-test Overall Self-Care score, N = 20, M = 0.55, SD = 0.51; post-test N = 20, M = 2.85, SD = 0.37), t(19) = -18.01, p < .05). This result is supported by a study done by Hunt (2015), which states that technology offers a platform where patients diagnosed with diabetes can be educated on new routines and practices related to diabetes management. The use of technology can support daily diabetes self-management activities which include problem-solving, monitoring for complications, taking medication, healthy eating, exercising, and blood glucose monitoring (Hunt, 2015).
The results of the project showed a favorable difference in glucose monitoring scores, physical activity, dietary control, overall health score, and increase in participant’s self-care scores on diabetes management of care. These findings were similar to the study of El-Gayar, Timsina, Nawar, and Eid (2013), which shows that implementation of smartphone applications, is linked with an enhanced attitude that favors diabetes self-management and the implementation of smartphone applications for diabetes self-management that would lead to improved health outcomes.
Implications and Conclusions
Diabetes self-management education is an essential element of care for all people with diabetes and those at risk of developing the disease. It is necessary to prevent or delay the complications of diabetes. According to the results of the project, it was determined that the implementation of the mobile-based DSME initiative is beneficial to the patients and healthcare providers at the Patient’s Choice Primary Care Associates Clinic. This was evident with the significant improvement in the glucose management, dietary control, physical activity, healthcare usage, and general self-care scores. The smartphones and applications offer a unique platform that can be utilized for communication where the applications can be integrated with healthcare information.
Nursing leaders are encouraged to find ways to incorporate mobile-health technology into their clinical standards of practice. The use of technology can be utilized to complement healthcare professionals to improve diabetes care by providing both motivational and educational support. According to the findings of the present study, integrating DSME and mobile technology, this new approach to diabetes management revealed that the implementation of diabetes self-management education and coaching might improve patient outcomes and the practice of nursing. Apart from nursing leaders, the results of this study are also significant to society as a whole. According to the International Diabetes Federation (IDF, 2018), in 2017, diabetes caused an estimated $727 billion in direct and indirect health expenditures. The IDF projects that this expenditure will increase significantly by 2045. As such, with a cost-effective alternative, a large part of society will benefit from this change in practice.
Recommendations
The current project highlights the importance of leveraging technology in the healthcare sector. Essentially, the findings depict that changing the current clinical practice in diabetes management to the utilization of mobile phones to deliver DSME/S has a positive impact on patient outcome. This is because the initiative improves the patient’s capacity to strictly adhere to the prescribed diabetes management plan.
Despite the fact that the findings of the present study established that mobile usage was beneficial to the patients, the adverse effects of the intervention were not explored because of the research limitation and use of 16 items in the pre- and post-implementation evaluations. Future research should focus on exploring the impact of the intervention in terms of benefits and adverse effects. This will require the use of robust pre- and post-implementation evaluation instruments. The concern over the adverse effects of a mobile intervention is not an isolated issue. There are several studies depicting the need to establish the adverse effects of mobile phone–based interventions in the clinical setting. A Cochrane systematic review conducted by Boels et al. (2017) highlights that there is limited evidence concerning the implementation of the mobile phone–based intervention. As such, future research should explore the adverse effects of using mobile phone–based interventions to deliver DSME/S.
References
American Diabetes Association. (2018). Classification and diagnosis of diabetes: Standards of medical care in diabetes. Diabetes Care, 41(1), 13–27.
Behar-Horenstein, L. S., Guin, P., Gamble, K., Hurlock, G., Leclear, E., Philipose, M.,… Weldon, J. (2005). Improving patient care through patient-family education programs. Hospital Topics, 83(1), 21–27. doi: 10.3200/HTPS.83.1.21-27
Boels, A., Vos, R., Metzendorf, M., & Rutten, G. (2017). Diabetes self-management education and support delivered by mobile health (m-health) interventions for adults with type 2 diabetes mellitus (Protocol). Cochrane Database of Systematic Reviews, 1–16. doi:10.1002/14651858.CD012869
Brunisholz, K. D., Briot, P., Hamilton, S., Joy, E. A., Lomax, M., Barton, N.,… Cannon, W. (2014). Diabetes self-management education improves quality of care and clinical outcomes determined by a diabetes bundle measure. Journal of Multidisciplinary Healthcare, 7, 533–542. doi:10.2147/JMDH.S69000
Burke, S. D., Sherr, D., & Lipman, R. D. (2014). Partnering with diabetes educators to improve patient outcomes. Diabetes, Metabolic Syndrome and Obesity: Targets and therapy, 7, 45–53. doi:10.2147/DMSO.S40036
Center for Disease Control and Prevention. (2018). Managing Diabetes. Retrieved from https://www.cdc.gov/learnmorefeelbetter/programs/diabetes.htm
Center for Disease Control and Prevention. (2019). Living with Diabetes. Retrieved from https://www.cdc.gov/diabetes/managing/index.html
Conget, I., Kirkman, M. S., Cao, D., Wong, M., & Kendall, D. M. (2017). Identifying insulin treatment responders with a composite measure: Beyond Hba1c <7% in patients with type 2 diabetes. Current Medical Research and Opinion, 34(2), 329–336. doi:10.1080/03007995.2017.1396968
Creswell, J. W., & Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approach. Los Angeles, CA: Sage.
Dabelea, D., Mayer-Davis, E. J., Saydah, S., Imperatore, G., Linder, B., Divers, J.,… Hamman, R. F. (2014). Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. Journal of the American Medical Association (JAMA), 311(17), 1778–1786.
Dick, J., Peek, M., Chou, C.-H., Nocon, R., Chin, M., & Peek, M. (2014). Mobile phone diabetes project led to improved glycemic control and net savings for Chicago plan participants. Health Affairs (Project Hope), 33(2), 265–272.
Dobson, R., Carter, K., Cutfield, R., Hulme, A., Hulme, R., McNamara, C., ...Whittaker, R. (2015). Diabetes text-message self-management support program (SMS4BG): A pilot study. JMIR Mhealth and Uhealth, 3(1), 32. doi:10.2196/mhealth.3988
El-Gayar, O., Timsina, P., Nawar, N., & Eid, W. (2013). Mobile applications for diabetes self-management: Status and potential. Journal of Diabetes Science and Technology, 7(1), 247–262.
Fitzner, K., & Moss, G. (2013). Telehealth—An effective delivery method for diabetes self-management education? Population Health Management, 16(3), 169–177.
Franc, S., Borot, S., Ronsin, O., Quesada, J., Dardari, D., Fagour, C., & Renard, E. (2014). Telemedicine and type 1 diabetes: Is technology per se sufficient to improve glycemic control? Diabetes and Metabolism, 40(1), 61–66.
Garabedian, L. F., Ross-Degnan, D., & Wharam, J. F. (2015). Mobile phone and smartphone technologies for diabetes care and self-management. Current Diabetes Reports, 15(12), 109. doi:10.1007/s11892-015-0680-8
Harris, T., Silva, S., Intini, R., Smith, T., & Vorderstrasse, A. (2014). Group diabetes self-management education in a primary care setting: A quality improvement project. Journal of Nursing Care Quality, 29(2), 188–193. doi:10.1097/NCQ.0b013e3182aa08b7
Holmen, H., Health, P., Wahl, A. K., & Småstuen, M. C. (2017). Tailored communication within mobile apps for diabetes self-management: A systematic review. Journal of Medical Internet Research, 19(6), 1–16.
Hunt, C. W. (2015). Technology and diabetes self-management: An integrative review. World Journal of Diabetes, 6(2), 225–233.
International Diabetes Federation. (2018). IDF diabetes atlas (8th ed.). Idf.org. Retrieved from https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html
International Telecommunication Union. (2013). The world in 2013: ITC facts and figures. Retrieved from http://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdf
Jackson, S. L. (2015). Research methods and statistics: A critical thinking approach. Belmont, CA: Cengage Learning.
Kim, T. K. (2015). T test as a parametric statistic. Korean Journal of Anesthesiology, 68(6), 540–546. doi:10.4097/kjae.2015.68.6.540
Lari, H., Noroozi, A., & Tahmasebi, R. (2018). Impact of short message service (SMS) education based on a health promotion model on the physical activity of patients with type II diabetes. Malaysian Journal of Medical Sciences, 25(3), 67–77.
Lavrakas, P. J. (2008). Encyclopedia of survey research methods. Thousand Oaks, CA: Sage.
Mitchell, G. (2013). Selecting the best theory to implement planned change. Nursing Management, 20(1), 32-7. Retrieved from http://search.proquest.com.proxy.chamberlain.edu/docview/1329184689?accountid=147674
National Institute for Health and Care Excellence. (2015). Type 1 diabetes in adults: Diagnosis and management. Retrieved from http://www.nice.org.uk/guidance/ng17
Nundy, S., Dick, J. J., Chou, C., Nocon, R. S., Chin, M. H., & Peek, M. E. (2014). Mobile phone diabetes project led to improved glycemic control and net savings for Chicago plan participants. Health Affairs (Project Hope), 33(2), 265–272. doi:10.1377/hlthaff.2013.0589
Orr, J. A., & King, R. J. (2015). Mobile phone SMS messages can enhance healthy behavior: A meta-analysis of randomized controlled trials. Health Psychology Review, 9(4), 397–416. doi: 10.1080/17437199.2015.1022847
Pender, N. (1996). Health promotion in nursing practice (3rd ed.). Stamford, CT: Appleton & Lange.
Pender, N., Murdaugh, C., & Parsons, M. (2011). Health promotion in nursing practice (6th ed.). Retrieved from http://www.r2library.com.proxy.lib.ohio-state.edu/marc_frame.aspx?ResourceID=2588
Pludwinski, S., Ahmad, F., Wayne, N., & Ritvo, P. (2016). Participant experiences in a smartphone-based health coaching intervention for type 2 diabetes: A qualitative inquiry. Journal of Telemedicine and Telecare, 22(3), 172–178. doi:10.1177/1357633X15595178
Powers, M. A., Bardsley, J., Cypress, M., Duker, P., Funnell, M. M., Fischl, A. H.,… Vivian, E. (2015). Diabetes self-management education and support in type 2 diabetes: A joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Journal of the Academy of Nutrition and Dietetics, 115(8), 1323–1334.
Ramachandran, A., Snehalatha, C., Ram, J., Selvam, C., Simon, M., Nanditha, A., … Johnston, D. G. (2013). Efficacy of mobile phone messaging in prevention of type 2 diabetes by lifestyle change in men at high risk—A randomized clinical trial in India. Lancet Diabetes Endocrinology 1(3), 191–198. doi: 10.1016/S2213-8587
Sandra, G. S., Omar, G., & Ruy, L.-R. (2009). Diabetes treatment and control: The effect of public health insurance for the poor in Mexico. Bulletin of the World Health Organization, 87, 512–519.
Santorelli, M., Ekanayake, R., & Wilkerson-Leconte, L. (2017). Participation in a diabetes self-management class among adults with diabetes, New Jersey 2013–2015. Preventing Chronic Disease, 14(E63), 1–5.
Schmitt, A., Gahr, A., Hermanns, N., Kulzer, B., Huber, J., & Haak, T. (2013). The Diabetes Self-Management Questionnaire (DSMQ): Development and evaluation of an instrument to assess diabetes self-care activities associated with glycemic control. Health and Quality of Life Outcomes, 11(1), 138.
Schmitt, A., Reimer, A., Hermanns, N., Huber, J., Ehrmann, D., Schall, S., & Kulzer, B. (2016). Assessing diabetes self-management with the diabetes self-management questionnaire (DSMQ) can help analyze behavioral problems related to reduced glycemic control. PloS One, 11(3), e0150774.
Shah, V. N., & Garg, S. K. (2015). Managing diabetes in the digital age. Clinical Diabetes and Endocrinology, 1(1), 16. doi:10.1186/s40842-015-0016-2
Slade, S., & Grad Dip, M. T. (2016, August 14). Diabetes management: Using eHealth in a Rural or Remote Setting. Retrieved from Joanna Briggs Institute Database (Accession No. JBI9244)
Tabák, A. G., Herder, C., Rathmann, W., Brunner, E. J., & Kivimäki, M. Prediabetes: A high risk state for diabetes development. The Lancet, 379(9833), 2279–2290.
Wall-Emerson, R. (2017). ANOVA and t-tests. Journal of Visual Impairment & Blindness, 111(2), 192–196. doi:10.1177/0145482X1711100214
Wangnoo, S. K., Maji, D., Das, A. K., Rao, P. V, Moses, A., & Sethi, B. (2013). Review article barriers and solutions to diabetes management: An Indian perspective. Indian Journal of Endocrinology and Metabolism, 17(4), 594–601.
Williams, J., & Cullen, L. (2016). Evidence into practice: Disseminating an evidenced-based practice project as a poster. Journal of Peri-Anesthesia Nursing, 31(5), 440-444.
Wojcicki, J. M., Ladyzynski, P., & Foltynski, P. (2013). What we can really expect from telemedicine in intensive diabetes treatment: 10 years later. Diabetes Technology and Therapeutics, 15(3), 260–268. doi:10.1089/dia.2012.0242


Evidence-Based Professionals' Monthly - July 2026

Evidence-Based Professionals' Monthly - June 2026

Evidence-Based Professionals' Monthly - May 2026

Evidence-Based Professionals' Monthly - April 2026

Evidence-Based Professionals' Monthly - March 2026

Evidence-Based Professionals' Monthly - February 2026

Evidence-Based Professionals' Monthly - January 2026

Evidence-Based Professionals' Monthly - December 2025
